Endoscopic Laryngology Education & Curriculum Enhancement for SLP Graduate Students
Find your school’s link below! If you wish for your institution to participate, kindly contact Liza Blumenfeld (liza@endo-education.com).


Heart Rate Variability
Stress. Anxiety. They are arguably two of the strongest negative experiences that we encounter personally and professionally. Sadly, we are often left helpless to mitigate the profound deleterious imprint of these emotions if they arise with frequency or become chronic. Stress and anxiety are often viewed as intangible emotions, disconnected from our physical state of being. Yet many report “stress” headaches or “anxious” stomachs. Consider that sharp twinge in your shoulders or neck every time your workload is on the brink of being unmanageable. Cohen, Kessler and Underwood (1995) define stress as “A process in which environmental demands tax or exceed the adaptive capacity of an organism, resulting in psychological and biological changes that may place persons at risk for disease.” The autonomic nervous system (ANS) is the thoroughfare responsible for filtering, processing, reacting to and recovering from stress. It contains two sub-components, the sympathetic nervous system (SNS) and parasympathetic nervous system (PNS). The SNS is traditionally referred to as the “fight or flight” stimulator. It triggers production of adrenaline and speeds up heart rate, allowing our bodies to rapidly react to acute, high stress situations. The PNS, or “rest and digest” system, helps restores a state of calm by reducing heart rate and stimulating our digestive system. A well regulated ANS maintains strong balance of SNS and PNS activity. When our systems are taxed by excess and prolonged stress, this balance is disrupted. Multiple publications have highlighted the negative impact of elevated SNS activity on GI, Cardiovascular and cognitive integrity. (Lucini et al, 2005)
As speech pathologists, we commonly encounter stress as a persistent triggering mechanism of many common pathologies such as cough, laryngospasm, muscle tension dysphonia and dysphagia. Yet, other than promoting insight and awareness of the correlation, clinicians historically have limited options to formally counteract stress reactivity. Various publications explore this relationship of stress and voice and swallowing ailments. Kim et al investigated the impact of diagnosed anxiety and depression prior to onset of head and neck cancer treatment. They found that individuals with these emotional disorders had significantly lower serum albumin levels, poorer pre-treatment quality of life scores and, astoundingly, reduction in 3-year disease free survival rates. Magnuson et al found prolonged reliance of PEG tubes and latency in return to baseline diet textures for post-chemoradiation patients. Stress and anxiety were reported as contributing factors to these lingering symptoms.
Dysphonia has strong roots in stress as well. Freidl (1990) reported significant correlation of etio-pathogenesis in functional voice disorders with stress and anxiety. Dietrich (2009) explored the relationships of stress, personality and hyperfunctional voice disorders. Results indicated that individuals with introverted personalities had a propensity for increased infrahyoid extralaryngeal muscle activity. They perceived greater vocal effort during speech, and this intensified with stress.
Clearly, stress and anxiety affect the disorders we treat. So how does heart rate variability biofeedback (HRVB) fit in as a therapeutic modality? To answer this question, one must re-examine the relationship that exists among the vagus nerve, stress reactivity and organ function. The central autonomic nervous system is a functional and structural network that integrates cognitive and affective processing with peripheral end organ activity. Prefrontal, limbic and brain stem regions communicate via the vagus nerve to tonically inhibit sympathetic innervation at rest and recover from stressors. Relentless exposure to stress, paired with high stress reactivity, may promote systemic vagal denervation and reduced vagal tone. The result can resemble a car that uncontrollably accelerates without an effective brake pedal. One may hypothesize that this phenomena, in concert with specific personality profiles, may predispose individuals for voice and swallowing disorders due to heightened levels of muscle tension and generalized hyper-responsiveness.
HRVB is evolving as a complementary modality in treatment of various ailments including depression, pain management and cardiovascular health. (Lehrer et al 2014). HRVB incorporates slow paced breathing with the primary end goal of stimulating maximum parasympathetic nervous system activity. The underlying mechanism lies in cardiorespiratory feedback training that supports and stimulates homeostasis in the baroreceptor (Vaschillo et al.,2002). This assists in recalibration of our autonomic system that allows for greater resilience in managing and processing stress. While the direct impact of HRVB in the management of voice and swallowing disorders lies in its infancy, the promise of improved stress tolerance for enhanced symptom management is enticing.
HRVB assessment requires specialized equipment that measures parameters of respiration, cardiac activity, temperature and skin condensation. It is completely non-invasive and can be easily incorporated within the formal speech pathology assessment period. Specialized protocols allow the clinician to identify the ideal respiratory and cardiac profile that maximizes PNS activity. This pattern is then habituated through a home exercise regimen that is performed daily via a mobile device application. Specialized training in HRVB assessment techniques is required in order to generate clinical proficiency. This process is minimally cumbersome. Behavioral response to HRVB includes a generalized sensation of calmness which allows clinicians to target desired outcomes, including cough suppression, breathing comfort, readiness for challenging dietary textures and vocal clarity.
Integration of HRVB into our clinical practice was serendipitous. The technique was introduced to us by a patient, a physician, seeking non-invasive and non-pharmacological resolution of his esophageal dysmotility and dysphonia. He was so impressed by his outcome, he felt compelled to share this therapeutic modality. We sought training from our psychology colleagues and began infusing HRVB into our practice. Our referring physicians were intrigued by this adjunctive therapy and suggested a retrospective analysis of HRVB clinical efficacy for hyperfunctional larynges. Symptoms were treated with HRVB as a complimentary measure to standard treatment. On average, patients underwent 2.9 sessions of skilled treatment prior to discharge. The majority of patients demonstrated elevated sympathetic nervous system activity during the baseline HRVB assessment. Patients demonstrated approximately 82% improvement in their systems as measures by behavioral assessments and tangible measures of cough activity. Participants also noted improvements in quality of life and psychological symptoms, such as stress and anxiety. These findings reflect significant improvements as compared to traditional treatment methods.
While the exact mechanisms of symptom improvement are not extractable from this early study, we hypothesized that HRVB restored ANS regulation and reestablished inefficient breathing patterns that may accompany laryngeal hyper-responsiveness. The technique also provided several patients with valuable insight into the relationship between cough behavior and psychological factors. Our clinical practice is currently performing two prospective studies exploring the utility of HRVB as a lone and/or complementary therapeutic modality in the management of chronic cough, dysphagia and generalized distress associated with head and neck cancer. Our goal is to further substantiate the role of stress reactivity and autonomic dysregulation in both dysphagia and dysphonia by objectively quantifying clinical improvement achieved through daily HRVB performance.
Psychological stress will invariably plague our patients’ daily lives. And we are unable to change personality traits lending to stress vulnerability. Providing patients the ability to override these factors with tangible parasympathetic “exercise” is a viable adjunctive method to reduce symptoms and improve quality of life.
Cohen, S., Kessler, R. C., & Underwood Gordon, L. (Eds.) (1995). Measuring stress: A guide for health and social scientist. New York: Oxford
Dietrich, Maria (2009) The effects of stress reactivity on extralaryngeal muscle tension in vocally normal participants as a function of personality. Doctoral Dissertation, University of Pittsburgh.
Freidl W1, Friedrich G, Egger J. (1990). Personality and coping with stress in patients suffering from functional dysphonia. (Article in German). Folia Phoniatr (Basel). 42(3):144-9.
Gevirtz, R. (2013). The Promise of Heart Rate Variability Biofeedback: Evidence-Based Applications. Biofeedback, 41(3), 110-120.
Lehrer, P. M., Vaschillo, E., Vaschillo, B., Lu, S., Scardella, A., Siddique, M., & Habib, R. H. (2004). Biofeedback Treatment for Asthma. Chest, 126(2), 352-361.
Lehrer, P., Vaschillo, E., Lu, S., Eckberg, D., Vaschillo, B., Scardella, A., & Habib, R. (2006). Heart Rate Variability Biofeedback. Chest, 129(2), 278-284.
Lupien, SJ., McEwen, BS., Gunnar, MR., Heim, C., (2009) The effects of stress throughout the lifespan on the brain, behavious and cognition. Nat Rev Neurosci. 434-45.
Heart Rate Variability
Stress. Anxiety. They are arguably two of the strongest negative experiences that we encounter personally and professionally. Sadly, we are often left helpless to mitigate the profound deleterious imprint of these emotions if they arise with frequency or become chronic. Stress and anxiety are often viewed as intangible emotions, disconnected from our physical state of being. Yet many report “stress” headaches or “anxious” stomachs. Consider that sharp twinge in your shoulders or neck every time your workload is on the brink of being unmanageable. Cohen, Kessler and Underwood (1995) define stress as “A process in which environmental demands tax or exceed the adaptive capacity of an organism, resulting in psychological and biological changes that may place persons at risk for disease.” The autonomic nervous system (ANS) is the thoroughfare responsible for filtering, processing, reacting to and recovering from stress. It contains two sub-components, the sympathetic nervous system (SNS) and parasympathetic nervous system (PNS). The SNS is traditionally referred to as the “fight or flight” stimulator. It triggers production of adrenaline and speeds up heart rate, allowing our bodies to rapidly react to acute, high stress situations. The PNS, or “rest and digest” system, helps restores a state of calm by reducing heart rate and stimulating our digestive system. A well regulated ANS maintains strong balance of SNS and PNS activity. When our systems are taxed by excess and prolonged stress, this balance is disrupted. Multiple publications have highlighted the negative impact of elevated SNS activity on GI, Cardiovascular and cognitive integrity. (Lucini et al, 2005)
As speech pathologists, we commonly encounter stress as a persistent triggering mechanism of many common pathologies such as cough, laryngospasm, muscle tension dysphonia and dysphagia. Yet, other than promoting insight and awareness of the correlation, clinicians historically have limited options to formally counteract stress reactivity. Various publications explore this relationship of stress and voice and swallowing ailments. Kim et al investigated the impact of diagnosed anxiety and depression prior to onset of head and neck cancer treatment. They found that individuals with these emotional disorders had significantly lower serum albumin levels, poorer pre-treatment quality of life scores and, astoundingly, reduction in 3-year disease free survival rates. Magnuson et al found prolonged reliance of PEG tubes and latency in return to baseline diet textures for post-chemoradiation patients. Stress and anxiety were reported as contributing factors to these lingering symptoms.
Dysphonia has strong roots in stress as well. Freidl (1990) reported significant correlation of etio-pathogenesis in functional voice disorders with stress and anxiety. Dietrich (2009) explored the relationships of stress, personality and hyperfunctional voice disorders. Results indicated that individuals with introverted personalities had a propensity for increased infrahyoid extralaryngeal muscle activity. They perceived greater vocal effort during speech, and this intensified with stress.
Clearly, stress and anxiety affect the disorders we treat. So how does heart rate variability biofeedback (HRVB) fit in as a therapeutic modality? To answer this question, one must re-examine the relationship that exists among the vagus nerve, stress reactivity and organ function. The central autonomic nervous system is a functional and structural network that integrates cognitive and affective processing with peripheral end organ activity. Prefrontal, limbic and brain stem regions communicate via the vagus nerve to tonically inhibit sympathetic innervation at rest and recover from stressors. Relentless exposure to stress, paired with high stress reactivity, may promote systemic vagal denervation and reduced vagal tone. The result can resemble a car that uncontrollably accelerates without an effective brake pedal. One may hypothesize that this phenomena, in concert with specific personality profiles, may predispose individuals for voice and swallowing disorders due to heightened levels of muscle tension and generalized hyper-responsiveness.
HRVB is evolving as a complementary modality in treatment of various ailments including depression, pain management and cardiovascular health. (Lehrer et al 2014). HRVB incorporates slow paced breathing with the primary end goal of stimulating maximum parasympathetic nervous system activity. The underlying mechanism lies in cardiorespiratory feedback training that supports and stimulates homeostasis in the baroreceptor (Vaschillo et al.,2002). This assists in recalibration of our autonomic system that allows for greater resilience in managing and processing stress. While the direct impact of HRVB in the management of voice and swallowing disorders lies in its infancy, the promise of improved stress tolerance for enhanced symptom management is enticing.
HRVB assessment requires specialized equipment that measures parameters of respiration, cardiac activity, temperature and skin condensation. It is completely non-invasive and can be easily incorporated within the formal speech pathology assessment period. Specialized protocols allow the clinician to identify the ideal respiratory and cardiac profile that maximizes PNS activity. This pattern is then habituated through a home exercise regimen that is performed daily via a mobile device application. Specialized training in HRVB assessment techniques is required in order to generate clinical proficiency. This process is minimally cumbersome. Behavioral response to HRVB includes a generalized sensation of calmness which allows clinicians to target desired outcomes, including cough suppression, breathing comfort, readiness for challenging dietary textures and vocal clarity.
Integration of HRVB into our clinical practice was serendipitous. The technique was introduced to us by a patient, a physician, seeking non-invasive and non-pharmacological resolution of his esophageal dysmotility and dysphonia. He was so impressed by his outcome, he felt compelled to share this therapeutic modality. We sought training from our psychology colleagues and began infusing HRVB into our practice. Our referring physicians were intrigued by this adjunctive therapy and suggested a retrospective analysis of HRVB clinical efficacy for hyperfunctional larynges. Symptoms were treated with HRVB as a complimentary measure to standard treatment. On average, patients underwent 2.9 sessions of skilled treatment prior to discharge. The majority of patients demonstrated elevated sympathetic nervous system activity during the baseline HRVB assessment. Patients demonstrated approximately 82% improvement in their systems as measures by behavioral assessments and tangible measures of cough activity. Participants also noted improvements in quality of life and psychological symptoms, such as stress and anxiety. These findings reflect significant improvements as compared to traditional treatment methods.
While the exact mechanisms of symptom improvement are not extractable from this early study, we hypothesized that HRVB restored ANS regulation and reestablished inefficient breathing patterns that may accompany laryngeal hyper-responsiveness. The technique also provided several patients with valuable insight into the relationship between cough behavior and psychological factors. Our clinical practice is currently performing two prospective studies exploring the utility of HRVB as a lone and/or complementary therapeutic modality in the management of chronic cough, dysphagia and generalized distress associated with head and neck cancer. Our goal is to further substantiate the role of stress reactivity and autonomic dysregulation in both dysphagia and dysphonia by objectively quantifying clinical improvement achieved through daily HRVB performance.
Psychological stress will invariably plague our patients’ daily lives. And we are unable to change personality traits lending to stress vulnerability. Providing patients the ability to override these factors with tangible parasympathetic “exercise” is a viable adjunctive method to reduce symptoms and improve quality of life.
Cohen, S., Kessler, R. C., & Underwood Gordon, L. (Eds.) (1995). Measuring stress: A guide for health and social scientist. New York: Oxford
Dietrich, Maria (2009) The effects of stress reactivity on extralaryngeal muscle tension in vocally normal participants as a function of personality. Doctoral Dissertation, University of Pittsburgh.
Freidl W1, Friedrich G, Egger J. (1990). Personality and coping with stress in patients suffering from functional dysphonia. (Article in German). Folia Phoniatr (Basel). 42(3):144-9.
Gevirtz, R. (2013). The Promise of Heart Rate Variability Biofeedback: Evidence-Based Applications. Biofeedback, 41(3), 110-120.
Lehrer, P. M., Vaschillo, E., Vaschillo, B., Lu, S., Scardella, A., Siddique, M., & Habib, R. H. (2004). Biofeedback Treatment for Asthma. Chest, 126(2), 352-361.
Lehrer, P., Vaschillo, E., Lu, S., Eckberg, D., Vaschillo, B., Scardella, A., & Habib, R. (2006). Heart Rate Variability Biofeedback. Chest, 129(2), 278-284.
Lupien, SJ., McEwen, BS., Gunnar, MR., Heim, C., (2009) The effects of stress throughout the lifespan on the brain, behavious and cognition. Nat Rev Neurosci. 434-45.
Phagophobia
Speech Pathologists in the medical environment spend the vast majority of the day evaluating and treating patients with Dysphagia. While the underlying etiology and presenting symptoms may vary, the therapeutic methodologies embrace overlapping themes. Less commonly, SLP’s are asked to alleviate swallowing difficulties in individuals with no detectable physiologic pathology as evidenced by objective testing. These patients are likely suffering from a rare condition known as phagophobia.
Phagophobia is a word that comes from Greek phagein, “eat” and phobos, “fear”. It is a fear of swallowing, expressed in various symptoms without any apparent physical reason detectable by physical inspection and clinical analyses. Other terms used to define this disorder include: functional dysphagia, choking phobia, pseudodysphagia and sitophobia. The most common complaints of the condition include difficulty with swallow initiation, abnormal oral behaviors, repetitive lingual movements, complaints of throat pressure and globus (Barofsky and Fontaine, 1998). The by-product of these symptoms functionally manifest in food/texture avoidance, severe anxiety, weight loss and malnutrition. Phagophobia is registered in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). The disorder is more common in females vs. males. Onset can range across the lifespan from childhood to geriatric. While incidence rates are extremely low, many patients are incorrectly diagnosed with this disorder and are later found to have an organic source of symptoms. The need to perform a comprehensive, multidisciplinary assessment is paramount in order to ensure that patients receive a correct diagnosis and restorative plan of care.
Some have equated the symptoms of phagophobia with those of a conversion disorder. The premise being that an individual subconsciously transforms psychological conflicts revolving around the act of eating, into somatic symptoms. Researchers have begun to challenge the historic notions of the disorder with clinical studies targeting brain function in these individuals. One study investigated cortical activity in patients suffering from phagophobia. They were able to identify objective changes in brain activity specifically in the insula, dorsolateral prefrontal cortex, and the premotor cortex of the R. Hemisphere. These represent the areas of the brain responsible for proprioception and coordination of temporal sequences and volitional oral-phase swallowing behaviors. (Sunstrup, 2014). Another interesting study by Leopold looked at broadening the traditional patterns of swallow sequencing beyond three phases. Their theory was that clinicians should integrate pre-oral and preparatory phases as part of the swallowing continuum. These crucial precursors to swallowing involve complex somatosensory inputs that can translate into altered motor programming. Patients who sustain repetitive negative stimuli/experiences relating to the act of swallowing may develop this complex disorder that manifests as phagophobia. These studies provide clinicians with heightened insight into the complexity of the condition and offer some clear direction regarding treatment. Unfortunately, there is a paucity of clinical efficacy studies highlighting treatment strategies to rehabilitate swallowing function in these individuals. Those that exist have extremely small sample sizes with limited SLP involvement. The vast majority identified combined methods of cognitive behavioral therapy (CBT) and exposure therapy as being the most effective tools in resolving symptoms of phagophobia. Historically, the role of SLPs in managing this disorder has been questionable. How do we address these patients’ unique complaints in the context of normal/intact swallowing physiology? In many cases, SLPs have opted to refer these patients to a mental health specialist under the premise that skilled dysphagia services were contraindicated. Today, SLPs are reevaluating this position and joining forces with mental health providers to offer patients therapy that addresses underlying swallowing anxieties in concert with oral-motor retraining and exposures to challenge foods and textures. This approach carries enormous promise as an efficacious therapeutic modality that restores normal eating/swallowing behavior through both cognitive and sensorimotor retraining.
Phagophobia
Speech Pathologists in the medical environment spend the vast majority of the day evaluating and treating patients with Dysphagia. While the underlying etiology and presenting symptoms may vary, the therapeutic methodologies embrace overlapping themes. Less commonly, SLP’s are asked to alleviate swallowing difficulties in individuals with no detectable physiologic pathology as evidenced by objective testing. These patients are likely suffering from a rare condition known as phagophobia.
Phagophobia is a word that comes from Greek phagein, “eat” and phobos, “fear”. It is a fear of swallowing, expressed in various symptoms without any apparent physical reason detectable by physical inspection and clinical analyses. Other terms used to define this disorder include: functional dysphagia, choking phobia, pseudodysphagia and sitophobia. The most common complaints of the condition include difficulty with swallow initiation, abnormal oral behaviors, repetitive lingual movements, complaints of throat pressure and globus (Barofsky and Fontaine, 1998). The by-product of these symptoms functionally manifest in food/texture avoidance, severe anxiety, weight loss and malnutrition. Phagophobia is registered in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). The disorder is more common in females vs. males. Onset can range across the lifespan from childhood to geriatric. While incidence rates are extremely low, many patients are incorrectly diagnosed with this disorder and are later found to have an organic source of symptoms. The need to perform a comprehensive, multidisciplinary assessment is paramount in order to ensure that patients receive a correct diagnosis and restorative plan of care.
Some have equated the symptoms of phagophobia with those of a conversion disorder. The premise being that an individual subconsciously transforms psychological conflicts revolving around the act of eating, into somatic symptoms. Researchers have begun to challenge the historic notions of the disorder with clinical studies targeting brain function in these individuals. One study investigated cortical activity in patients suffering from phagophobia. They were able to identify objective changes in brain activity specifically in the insula, dorsolateral prefrontal cortex, and the premotor cortex of the R. Hemisphere. These represent the areas of the brain responsible for proprioception and coordination of temporal sequences and volitional oral-phase swallowing behaviors. (Sunstrup, 2014). Another interesting study by Leopold looked at broadening the traditional patterns of swallow sequencing beyond three phases. Their theory was that clinicians should integrate pre-oral and preparatory phases as part of the swallowing continuum. These crucial precursors to swallowing involve complex somatosensory inputs that can translate into altered motor programming. Patients who sustain repetitive negative stimuli/experiences relating to the act of swallowing may develop this complex disorder that manifests as phagophobia. These studies provide clinicians with heightened insight into the complexity of the condition and offer some clear direction regarding treatment. Unfortunately, there is a paucity of clinical efficacy studies highlighting treatment strategies to rehabilitate swallowing function in these individuals. Those that exist have extremely small sample sizes with limited SLP involvement. The vast majority identified combined methods of cognitive behavioral therapy (CBT) and exposure therapy as being the most effective tools in resolving symptoms of phagophobia. Historically, the role of SLPs in managing this disorder has been questionable. How do we address these patients’ unique complaints in the context of normal/intact swallowing physiology? In many cases, SLPs have opted to refer these patients to a mental health specialist under the premise that skilled dysphagia services were contraindicated. Today, SLPs are reevaluating this position and joining forces with mental health providers to offer patients therapy that addresses underlying swallowing anxieties in concert with oral-motor retraining and exposures to challenge foods and textures. This approach carries enormous promise as an efficacious therapeutic modality that restores normal eating/swallowing behavior through both cognitive and sensorimotor retraining.
High Resolution Manometry to Manage Complex Dysphagia
Course Description
This presentation reviews how high-resolution manometry (HRM) transitioned from a research technology to a clinical tool. The opportunity to measure pressures may provide the clinician a more complete profile for planning treatment for patients with complex dysphagia. Case examples are presented to demonstrate the opportunities manometry offers to investigate pressure events during swallowing.
Time ordered agenda
15 minutes – Evolution of HRM for oral-pharyngeal disorders
15 minutes – Techniques and competencies to perform HRM
15 minutes – Case studies
15 minutes – Question and answer
Learning Objectives
1) Describe how HRM permits visualization of the pharynx amid 12 sensors.
2) Develop protocol for GI collaboration and training to integrate HRM for oral-pharyngeal disorders.
3) Verbalize patient populations for which HRM is inappropriate.
Disclosures
Molly Knigge, MA, CCC-SLP, BCS-S
Financial: Employed at University of Wisconson Madison Medical Center
Non-Financial: Nothing to disclose
![]()
iVoiceTherapy Webinar 2.12.15
Course Description:
This webinar is designed for clinicians to develop care programs for hypophonia within iVoiceTherapy. It is also applicable for any neurogenic disturbance altering other speech subsystems. Features to enhance compliance with these populations include the built in sound level meter, pitch monitor, journal, voice recorder and audio exercises. Specific case examples will reflect therapeutic strategies based on medical history. Should you be unavailable on the scheduled webinar date, this course will available at endo-education.com/online-ceus/ until 2.12.16. Course 0041. 0.1 ASHA CEUs. (Introductory level; Professional area).
Time ordered agenda:
12:00 – 12:15 Patient selection: PD stage, stimulability, family support.
12:15 – 12:30 Programming tasks and exercises
12:30 – 12:45 Case studies
12:45 – 13:00 Question and Answer
Learning Objectives
1) Verbalize appropriate candidates for voice therapy and iVT use to augment care of Parkinson’s disease.
2) Predict timeline of improvement with combination of in-person and iVT care plans.
3) Independently program exercises, alarms, voice files and settings in iVT for Parkinson’s patients.
Disclosures:
This presentation will focus solely on the product iVoiceTherapy and will not include information on other similar or related products.
Liza Blumenfeld
Financial: Partnership with Sinnova, which receives royalties from sale of iVoiceTherapy.
Non-financial: Owner of Endo Education, host of iVoiceTherapy training.
Erin Walsh
Financial: Partnership with Sinnova, which receives royalties from sale of iVoiceTherapy.
Non-financial: Owner of Endo Education, host of iVoiceTherapy training.
![]()
| |
POST-TEST, COURSE EVALUATION, CEUs, PRINT CERTIFICATE
Aspiration Pneumonia in Patients with Dysphagia
Course Description
This hour webinar was hosted by the National Foundation of Swallowing Disorders and featured Tiffany Mohr, a medical speech pathologist, with extensive experience in complex swallowing disorders. It is appropriate for introductory level clinicians seeking review of lung physiology, phases of swallowing and risk factors for aspiration developing into a pneumonia. Ms. Mohr provides guidance on other types of pneumonia and how they are distinctly different from those related to aspiration. She discusses aspiration risks based on specific populations including stroke and cancer. The webinar concludes with a 30 minute question and answer session. The audience was a mixture of patients, caregivers and speech pathologists.
Time ordered agenda
15 minutes – Basic lung function and swallow physiology.
10 minutes – Pneumonia acquisition.
5 minutes – Medical co-morbidities and aspiration pneumonia.
30 minutes – Question and answer
Learning Objectives
1) Describe normal reflex when foreign material enters lungs.
2) Differentiate types of pneumonia and how each are acquired.
3) Verbalize 3 risk factors for development of aspiration pneumonia.
Disclosures
Tiffany Mohr, MA, CCC-SLP
Financial: Nothing to disclose
Non-Financial: Nothing to disclose
![]()
Masood Mansour, MD
 Presenter: Masood Mansour, MD, GastroenterologistCoastal Gastroenterology & Scripps Center for Voice, Swallowing and MotilityDr. Mansour graduated from UCLA David Geffen School of Medicine in 2007. Upon completion of Internal Medicine and Gastroenterology residencies at Scripps Clinic, he developed interests in esophageal manometry and pH testing. In 2014, he joined Scripps Center for Voice, Swallowing & Motility where he conducts a weekly multidisciplinary clinic with speech-language pathologists. Cases seen at the clinic include reflux, irritable larynx, pharyngeal and esophageal dysphagia, cough, achalasia and esophageal spasms. Dr. Mansour performs esophagogastroduodenoscopy, high resolution manometry, impedance and pH testing to diagnose their conditions and develop care plans. He works closely with a laparoscopic surgeon and periodically refers patients for myotomies, fundoplications and LINX procedures.
Presenter: Masood Mansour, MD, GastroenterologistCoastal Gastroenterology & Scripps Center for Voice, Swallowing and MotilityDr. Mansour graduated from UCLA David Geffen School of Medicine in 2007. Upon completion of Internal Medicine and Gastroenterology residencies at Scripps Clinic, he developed interests in esophageal manometry and pH testing. In 2014, he joined Scripps Center for Voice, Swallowing & Motility where he conducts a weekly multidisciplinary clinic with speech-language pathologists. Cases seen at the clinic include reflux, irritable larynx, pharyngeal and esophageal dysphagia, cough, achalasia and esophageal spasms. Dr. Mansour performs esophagogastroduodenoscopy, high resolution manometry, impedance and pH testing to diagnose their conditions and develop care plans. He works closely with a laparoscopic surgeon and periodically refers patients for myotomies, fundoplications and LINX procedures.
Case: Healthy 19yo male with 10 month history of chest pain, nausea, vomiting and dysphagia. He struggles to consume both liquids and solids, resulting in a 30lb weight loss. Trial of PPI and Reglan did not improve his symptoms. EGD 4 weeks ago revealed mild gastritis. Biopsies were normal. Esophagram demonstrated poor lower esophageal sphincter relaxation.
PMH: Generally unremarkable. Ear infections.
Social: Sophmore in college.
High Resolution Manometry:
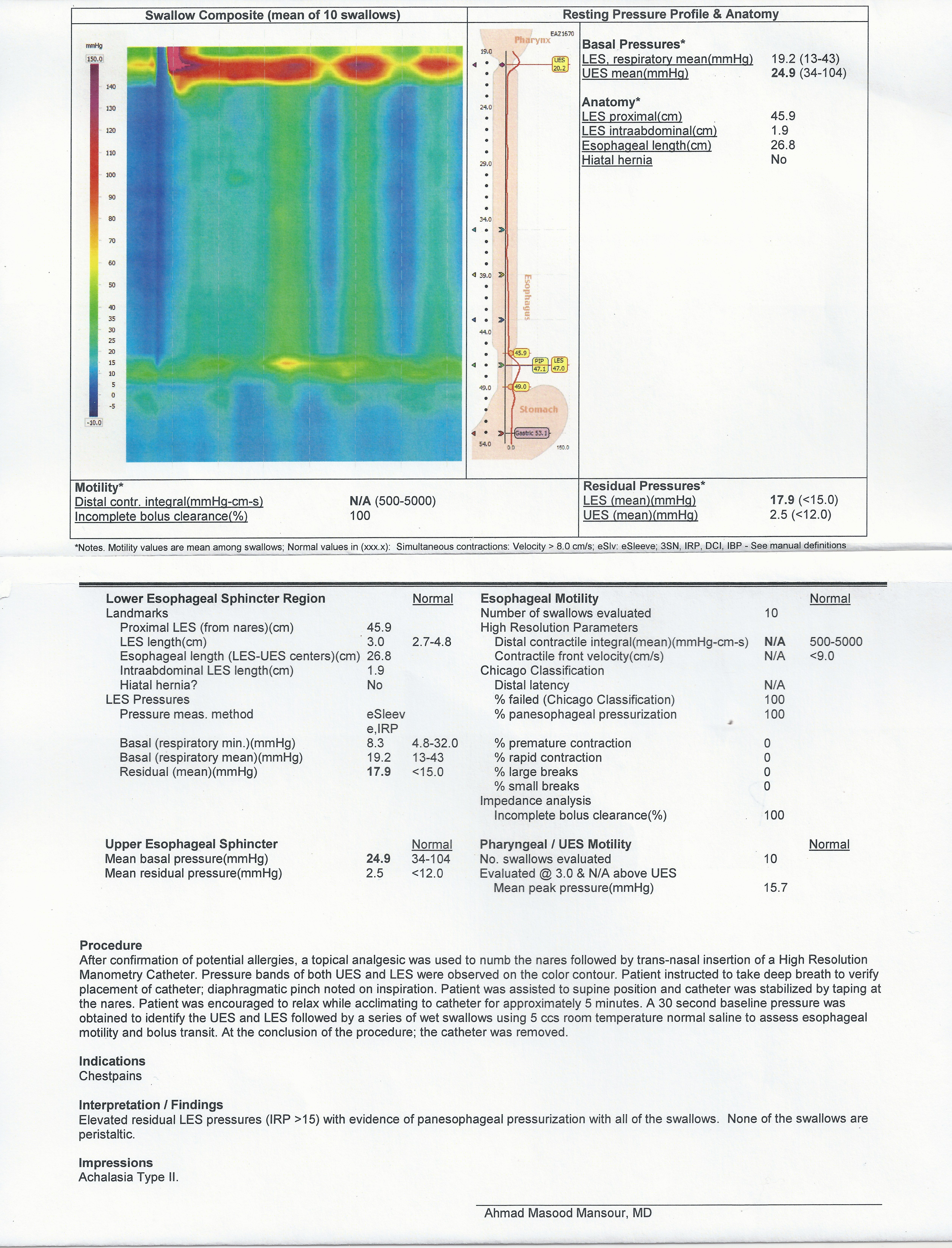
Treatment: Discussed with patient and his family variety of options to manage his condition. 1) Botox – not recommended due to age and need for repeat injections 2) Pneumatic dilation – norms for good response to this therapy are on females older than 45. There is risk of perforation and it is likely repeat dilations will be required. 3) Myotomy with partial fundoplication – long-term solution to his condition. This was the recommended course of therapy. Risk of post-operative reflux was discussed. After speaking with the laparoscopic surgeon, the family ultimately decided on option #3.
Surgery: Uncomplicated laparoscopic esophageal Heller myotomy with Dor fundoplication. Initiated a soft diet on post-op day 1. Mild abdominal epigastic tenderness and discomfort so on post-op day 2 underwent esophagram to assure no leak. The study revealed no obstruction and no Gastrografin leak. He was discharged home on post-op day 2.
Outcome: 11 days after surgery feels well, no fatigue or pain. Nausea and vomiting resolved. He is able to eat and drink anything. Although he has not gained weight, he exhibits an appropriate body mass index. Prior to developing achalasia, he was approximately 20lbs overweight.
Ever wish you could ride on your patient’s shoulder?
We all know that the rise and influence of mobile technology is astounding. Our smart phones are extrinsically becoming an extension of ourselves. Our smart phones have allowed us to do everything from listen to specially tailored radio stations to monitoring our daily calories and movement patterns. The power of this technology is extraordinary. It allows for immediate and constant access to the services and interests that we select. It is not surprising that the power of mobile app technology has been well integrated into the healthcare arena. Patients are now able to monitor their heart rates, check their blood sugar levels and get daily reminders to take their medications. Preliminary research studies have validated that patients are more likely to demonstrate compliance and clinical advancement with use of this technology. It is a powerful vehicle to maintain strong contact between the patient and the medical provider. The most recent wave of applications has now taken residence within the world of skilled voice therapy.
iVoiceTherapy is designed to provide clinicians with a unique opportunity to customize a dedicated voice therapy home exercise regimen in an educational and engaging format. It is perfect for all individuals seeking restoration of speaking or singing voice quality. The application blends core elements that translate into optimal levels of patient compliance. They include, exercise programming/cueing, patient education and biofeedback. Clinicians are able to program various settings that will cue patients to perform specific exercises at designated times. Patients’ receive visual and auditory messages prompting the performance of tasks. After completion, each encounter is time dated and stamped for subsequent review with the treating clinician.
iVoiceTherapy offers patients the ability to view and explore a gallery of laryngeal pathologies as well as a broad array of educational materials designed to promote enhanced awareness and overall level of engagement. It allows patients to visualize the nature of their impairments as a way of reaffirming their commitment to voice restoration. Similarly, iVoiceTherapy employs a variety of aids to foster understanding and subsequent compliance with designated behaviors to improve laryngeal hygiene and posture.
The application is well suited for individuals who sustain acute or chronic voice changes associated with a broad array of diagnoses including traumatic vocal fold lesions, muscle tension dysphonia, Irritable larynx syndrome as well as professional and avocational singers. iVoiceTherapy is designed to be a physician and clinician driven platform that is specially tailored by the medical team. Clinicians are able to identify patients who would benefit from the regimen and suggest download from the iTunes store. Once downloaded, the application will be programmed by the treating clinician to ensure that all salient issues are addressed. Patients are instructed to perform exercises and document progress on a daily basis. This allows both parties to review progress during subsequent visits. The application is fluid in that it can be reprogrammed in order to assist with progression towards stated goals.
iVoiceTherapy also serves as an excellent desk reference for clinicians who encounter voice disorders less frequently. The ear training and pathology labs permit familiarity with the most commonly encountered voice conditions. Navigation through the Exercises tab provides auditory modeling of resonant voice therapy, paradoxical vocal fold movement strategies, cough suppression, flexibility/strengthening tasks and singing regimens.
iVoiceTherapy is currently available on the iTunes store for $12.99. It is optimized for an iPhone. The application will also work on an iPad.
Motility Disorders in Dysphagia and Dysphonia
Speech Pathologists routinely encounter patients who present with well-defined voice and swallowing disturbances fueled by motility disorders. However, capturing objective information about esophageal function can often be difficult and frustrating for both the patient and the clinician. There are a variety of reasons for this: 1. There are a limited number of Otolaryngologists and Gastroenterologists that specialize in esophageal motility 2. Technology that evaluates these disorders is expensive and requires specialty-trained staff. 3. Motility testing is rarely housed within a dedicated voice and swallowing center which creates a challenge in multidisciplinary collaboration and communication.
Understanding the role of motility disorders in co-existing dysphagia and dysphonia is imperative. The esophagus is a muscular tube that extends from the neck to the abdomen and connects the back of the throat to the stomach. The upper and lower most segments are high-pressure sphincters that are tonically contracted at rest and provide protection against back flow of material. When a person swallows, the coordinated muscular contractions of the esophagus propel the food or fluid from the throat to the stomach. If the muscular contractions become disrupted or weak, patients may experience a variety of symptoms. Acid regurgitation may or may not be reported. Patients may come into the speech pathology clinic complaining of chronic, refractory cough, persistent dysphonia and laryngospasm, as of which may be directly fueled or exacerbated by motility disorders.
High resolution manometry is an invaluable tool that allows for detailed evaluation of pressure and motor function within the esophagus and can help in diagnosing complex disorders including: GERD/LPR, Hiatal Hernia, Nutcracker esophagus and Achalasia. pH testing similarly generates objective quantification of reflux events that occur over an extended period of time. Together, these tools provide the SLP with essential information that allows for the most accurate assessment and understanding of complex voice and swallowing disorders. It also allows for sound, mutli-disciplinary treatment planning in order to generate the most ideal clinical outcomes. -Liza Blumenfeld
Alternative singing styles can be perfectly healthy
Recently I had the pleasure of working with a brilliant woman enjoying a successful singing career as an avante-garde performer with trademark vocal acrobatics and multiphonics. Through experimentation, she taught herself to produce different tones simultaneously. Once you listen to her unusual vocal style, you may assume misuse generated her referral. Not so. And I am certainly in no place to advise her to discontinue a performance style she is passionate about and has never left a shred of vocal pathology. On the contrary, I was grateful to learn from her skill to share with other vocalists how to safely produce tones some may classify as screaming. I have seen these produced in unhealthy manners with devastating after effects, namely hemorrhaging and vocal cord scarring. A singing sample and her laryngeal videostroboscopy are provided below. There two aspects of her endoscopy you may find intriguing. First, her vocal cords are in pristine condition. They are pearly white and exhibit healthy edges. The edges of the vocal cords are generally where a pathology would arise from overuse due to repeated forceful closure. Secondly, when I ask her to reproduce simultaneous pitches, you will notice she elicits two vibrations in different quadrants of the vocal cords. Generally, we see one vibratory collision involving the entire true vocal cord. I was grateful for this opportunity to work with such an energetic performer and explore the technical skill of her vocal style. -Erin Walsh
Newsletter

Medicare Therapy Cap:
What patients and clinical service providers need to know.
Background: The “Balanced Budget Act of 1997” imposed a $1,500 cap on outpatient therapy services. Section 4541 (c) and (d) of the act increased the financial limitation to no more than $1500 of the incurred expenses in a calendar year, and applied it to outpatient therapy services furnished in skilled nursing facilities, physician’s offices, home health agencies (Part B), skilled nursing facilities (Part B), in addition to private practice offices. This cap did not apply to hospital-based outpatient programs. The effective date of this $1,500 cap was January 1, 1999. A myriad of legal actions were successful in delaying implementation of the cap, until it cleared all barriers and went into effect on January 1st, 2006. Later that year, congress generated legislation that created an exception process, thereby allowing continued care for specified patients that have exceeded the cap.
In early 2012, President Obama signed into law The Middle Class Tax Relief and Job Creation Act (H.R. 3630). This legislation mandated that Hospital-based outpatient would be subject to the therapy cap process beginning in October, 2012.
Unless legislation is passed, Beginning on January 1st, 2013, the exceptions process will no longer be in effect and all outpatient therapy settings, excluding hospital based outpatient programs, will be forced to strictly adhere to the therapy cap provisions.
Understanding the current process:
The current therapy cap amount is $1800 for Speech Therapy and Physical Therapy combined. It is unclear as to why two disciplines share the cap amount. Through the exceptions process, patients may receive additional services in excess of the cap, if clinicians identify continued need for skilled therapy. In 2012, there are two exception processes: an automatic exception and a manual medical review process. The automatic exception to the therapy cap can be utilized to extend patients’ services from $1880 to $3700. No prior authorization is required, however, by continuing treatment, clinicians are attesting that the services billed are: 1. Qualified for the cap exception, 2. Are reasonable and necessary services that require the skills of a therapist and 3. Are justified by appropriate documentation in the medical record. The manual medical review process is required for all patients who reach $3700 in reimbursed services. The process will require that clinicians obtain advanced approval from Medicare. Criteria for medical review will be based on current medical review standards. Clinicians must comply with coverage, documentation and coding requirements set forth in the Medicare Benefit Manual (Publication 100-02, chapter 15, section 220) and the Medicare Administrative Contractor (MAC) local coverage determination (LCD) for their jurisdiction.
Patient Corner
What are the outpatient therapy limits for 2012?
- $1,880 for physical therapy (PT) and speech-language pathology (SLP) services combined
- $1,880 for occupational therapy (OT) services After you pay your yearly deductible for Medicare Part B (Medical Insurance), Medicare pays its share (80%), and you pay your share (20%) of the cost for the therapy services. The Part B deductible is $140 for 2012. Medicare will pay its share for therapy services until the total amount paid by both you and Medicare reaches either one of the therapy cap limits. Amounts paid by you may include costs like the deductible and coinsurance.
What can I do if I need services that will go above the outpatient therapy cap amounts?
- You may qualify to get an exception to the therapy cap limits so that Medicare will continue to pay its share for your therapy services. Your therapist must document your need for medically-necessary services in your medical record, and your therapist’s billing office must indicate on your claim for services above the therapy cap that your outpatient therapy services are medically necessary. Even if your therapist provides documentation that your services were medically necessary, you might still have to pay for costs above the $1,880 therapy cap limits. If Medicare finds, at any time (even after your therapy services have been paid for), that the services above the therapy cap limits weren’t medically necessary, you might have to pay for the total cost of the services above the $1,880 therapy cap limits. Starting October 1, 2012, a Medicare contractor may review your medical records to check for medical necessity if you got outpatient therapy services in 2012 higher than these amounts: $3,700 for PT and SLP combined. $3,700 for OT Note: The Medicare contractor may conduct this review of your medical records before you get any additional outpatient therapy services.
How can I find out if my therapy services will go above the therapy cap limits?
- Ask your therapist’s billing office. If you get all your therapy in the same place, your therapist’s billing office will have the most up-to-date information and will know if your services will go above these limits.
- Visit www.MyMedicare.gov to track your claims for therapy services. This website is Medicare’s secure online service for accessing your personal Medicare information.
- Check your “Medicare Summary Notice” (MSN). This is the notice you get in the mail (usually every 3 months) that lists the services you had and the amount you may be billed.
What is an ABN?
- An ABN is an Advanced Beneficiary Notification. You may be asked by your clinical provider to sign this form prior to receipt of therapy services. The form states that in the event your services are not covered under medicare, you (The patient) will become responsible for payment. It is important to ensure that the provider includes a specific monetary amount that you would be billed. You should maintain a copy of this report for your personal records